Despite PMJAY’s cashless promise, high out-of-pocket expenditure and private sector gaps persist; achieving true Universal Health Coverage requires increasing public health funding to 2.5% of GDP, stricter private healthcare regulation, and adopting centralized, efficient medicine procurement models.

Copyright infringement not intended
Picture Courtesy: INDIANEXPRESS
Why In News?
A NITI Aayog study highlighted that the high Out-of-Pocket Expenditure (OOPE) in private hospitals undermines Pradhan Mantri Jan Arogya Yojana (PMJAY) goal of providing financial security to vulnerable families.
What are the Key Findings of the NITI Aayog Study?
Cost Disparities in Healthcare
|
Patient Category |
Average OOPE in Public Hospitals |
Average OOPE in Private Hospitals |
|
PMJAY Beneficiary |
Rs 21,827 |
Rs 53,965 |
|
Non-Insured Patient |
- |
Rs 74,847 |
Key Insights from the Study
Why is Out-of-Pocket Expenditure Still High?
Exclusion of Indirect Costs
The scheme does not cover costs like patient transport to and from hospitals, which places a heavy burden on rural families travelling to urban centres for tertiary care.
Gaps in Public Infrastructure: Public hospitals often face stock-outs of essential medicines and lack advanced diagnostic equipment.
Private Sector Practices: Private hospitals often engage in practices like upselling non-covered services or unbundling packages to charge patients extra.
Chronic Underfunding of Health: Indian government health expenditure is just 1.9% of GDP. (Source: Budget 2025-26).
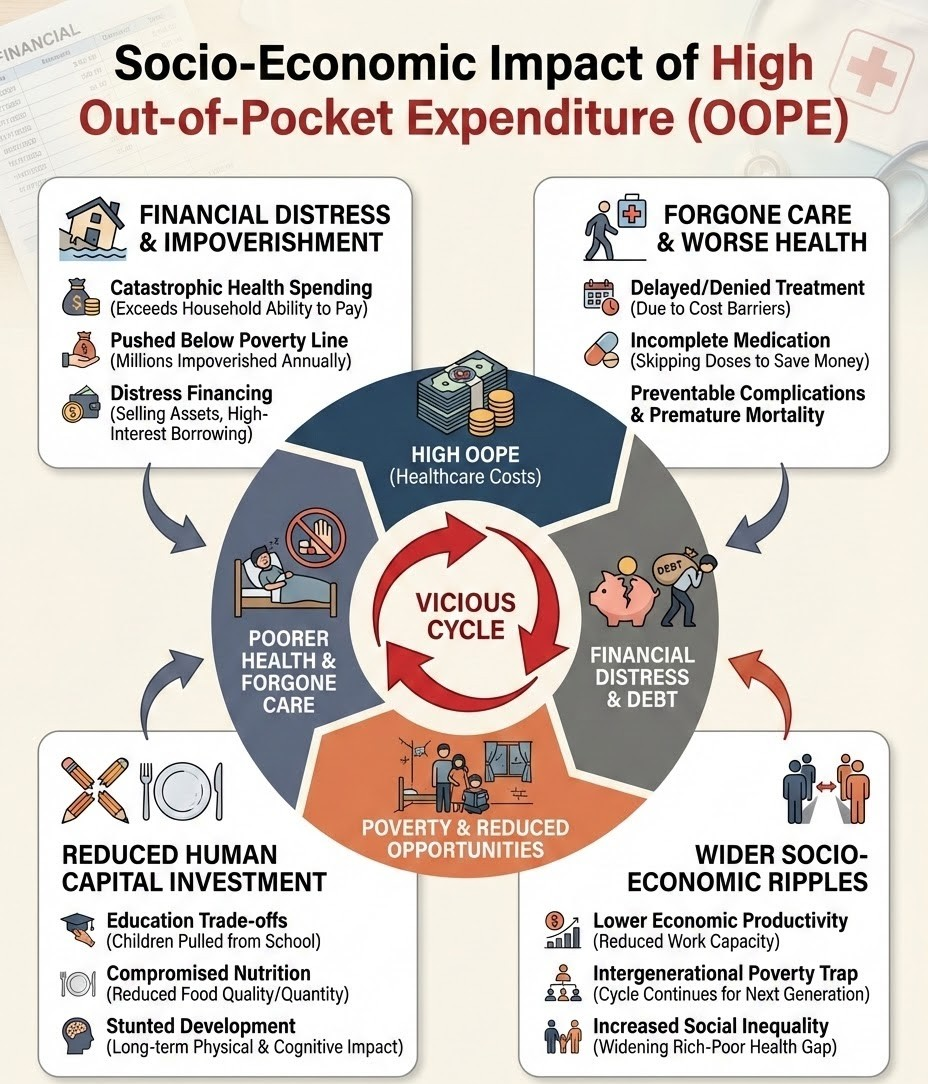
Socio-Economic Impact of High OOPE
Catastrophic Health Expenditure (CHE)
High OOPE pushes households into poverty. The World Bank estimates that such expenses push nearly 100 million people into extreme poverty globally each year.
Debt Cycles
Families often resort to distress borrowing or selling productive assets (like land or livestock) to fund surgeries or chronic care, leading to long-term intergenerational debt.
Undermining Universal Health Coverage (UHC)
A key goal of UHC is to reduce financial hardship. India remains far from the expert-recommended target of reducing OOPE to below 20% of total health spending.
Delayed Care-Seeking
High costs force individuals to delay seeking treatment for early symptoms, leading to complications and higher mortality rates.
Gender Disparity
Studies indicate that households are less likely to incur high OOPE for female members compared to males, exacerbating gender-based health inequities.
The "Missing Middle"
While the poorest 40% are covered by Ayushman Bharat and the top 10% have private insurance, nearly 40 crore people in the "middle" remain uninsured and highly vulnerable to OOPE shocks. (Source: NITI Aayog)
Way Forward
Expand the Benefit Package
Integrate essential non-medical costs like transport allowances into the PMJAY package, similar to the model used in the Janani Suraksha Yojana (JSY).
Adopt Centralized Procurement
States must replicate the successful Tamil Nadu model to ensure an uninterrupted supply of free generic medicines and diagnostics in all public hospitals.
Regulate Private Providers
Enforce the Clinical Establishments Act, 2010 strictly to standardize costs and prevent unethical practices like upselling and overcharging by private hospitals.
Increase Public Health Spending
The government must meet its commitment to increase public health expenditure to 2.5% of GDP by 2025 as stated in the National Health Policy 2017.
Learning From Best Practices
Domestic Model: Tamil Nadu Medical Services Corporation (TNMSC)
Global Model: Thailand’s Universal Coverage Scheme (UCS)
Conclusion
To ensure PMJAY fulfills the constitutional mandate of the Right to Health under Article 21, the government must transition from a limited insurance model to a comprehensive 'health assurance' framework that eliminates high out-of-pocket expenditure (OOPE) by expanding benefit packages, regulating private sector costs, and strengthening public primary healthcare.
Source: INDIANEXPRESS
|
PRACTICE QUESTION Q. "Despite being the world's largest health assurance scheme, PMJAY struggles to eliminate out-of-pocket expenditure (OOPE) for its beneficiaries." Analyze. 150 words |
The study revealed that despite PMJAY's cashless promise, beneficiaries still incur high Out-of-Pocket Expenditure (OOPE), averaging Rs 53,965 in private hospitals, meaning the scheme only provides marginal financial savings compared to uninsured patients.
High OOPE is driven by the exclusion of indirect costs like transportation, frequent stock-outs of essential medicines and diagnostics in public hospitals, and the private healthcare sector's tendency to upsell upgraded services or unbundle packages.
The Tamil Nadu Medical Services Corporation (TNMSC) model utilizes centralized bulk procurement and a robust IT-backed logistics system to ensure public hospitals are fully stocked with free generic medicines, reducing the OOPE burden on patients.

© 2026 iasgyan. All right reserved